2.1 Epidemiology
The following are the types of questions prenatal epidemiologists might ask:
 What factors influence seeking and receiving prenatal care, a known determinant for improving fetal outcomes?
What factors influence seeking and receiving prenatal care, a known determinant for improving fetal outcomes?- How do social gradients in the prenatal period affect fetal short- and long-term outcomes?
- What factors promote healthy nutritional behaviours during the preconception and prenatal periods?
The findings from this type of research can inform policy and health sector decision makers related to health promotion and illness and injury prevention strategies, potentially improving future child development and influencing health at a population level.
Read one woman’s story on the next link to the Maternity Worldwide website.
What stood out for you from Ayantu’s story?
Currently, the WHO (2016) recommends attending at least eight prenatal care visits. What are some barriers that might make this challenging for some people who are pregnant?
Epidemiology is the study of the distribution and determinants of health-related states or events (including disease), and the application of this study to the control of diseases and other health problems. Various methods can be used to carry out epidemiological investigations: surveillance and descriptive studies can be used to study distribution; analytical studies are used to study determinants” (WHO, n.d.-c).
For example, the maternal mortality rate rose in 2021 by 40,000 more maternal deaths from 2020. It is possible that the COVID-19 pandemic contributed to this via two mechanisms-pregnant individual who had SARS-CoV-2 infection and died as a result of the interaction between COVID-19 and their pregnant state; and/or a disruptions to health services hindered by access to and/or quality of care resulting in pregnancy complications that ended in mortality, when they may otherwise have been prevented or managed successfully (Calvert et al., 2021).
Data about maternal health has been collected and analyzed from various regions around the world. Revealing statistics about disease, contraception, prenatal care services, caesarean births, and attendance at birth by skilled health personnel are presented below on the WHO’s Global Health Observatory data repository. Explore the various maternal health topics in the link below.
Scroll down the table on the link above to find the country where you live and its associated data. What can you tell from this data about health services coverage for the region where you live?
What do you notice generally about these statistics for higher versus lower income countries?
Prenatal care
To achieve –The Every Woman Every Child vision and the Global Strategy for Women’s, Children’s and Adolescents’ Health, — we need innovative, evidence-based approaches to antenatal care” (WHO, 2016, p. 4).
Watch the next two videos as Dr. Maggie Morris, professor, Department of Obstetrics, Gynecology and Reproductive Sciences, University of Manitoba, explains the value of prenatal care from her medical perspective and terms associated with pregnancy outcomes.
The next two readings are on the WHO website. Read first about the social determinants of health to discover more about the “social gradient” and how socioeconomics can impact health and outcomes within and between populations.
For current WHO statistics and data on maternal mortality, read the next media Maternal Mortality fact sheet. Discover more about the main barriers to prenatal care in the section “Why do women not get the care they need?”
Currently, WHO (2016) recommends prenatal care from previous four contacts to eight contacts in pregnancy. Evidence shows that more frequent contact with health providers is linked to fewer stillbirths and better pregnancy outcomes, largely because it allows for earlier detection and management of complications. The expanded model could reduce perinatal deaths by up to 8 per 1,000 births compared to the previous four-visit approach
Unlike a simple “visit,” a “contact” refers to ongoing, meaningful interactions and care between the pregnant individual and health care provider. The schedule includes contacts at ≤12, 20, 26, 30, 34, 36, 38, and 40 weeks. However, if a pregnant individual has health conditions before pregnancy or develops health conditions that could adversely impact the pregnancy then, these contacts will be more frequent than eight contacts.
The WHO guideline also emphasizes that each contact should include comprehensive care, such as health education, nutrition counselling, screening tests, vaccinations, ultrasound and fetal assessment, and management of common pregnancy symptoms. Overall, the goal is to improve early risk detection, strengthen communication, and support healthier maternal and fetal outcomes (WHO, 2016).
There are variations between countries about the recommended number of prenatal contacts. In Canada, consistent with SOGC-informed care, prenatal visits typically occur every 4–6 weeks in early pregnancy, increase to every 2–3 weeks in the third trimester, and become weekly after 36 weeks’ gestation (Public Health Agency of Canada, 2026). In the next video, Dr. Maureen Heaman talks about her research which revealed geographic variations in access to prenatal care within the province of Manitoba, Canada.
Listen as Heaman explains how further research identified other population factors linked with inadequate prenatal care.
Look at the following graph from the Manitoba Centre for Health Policy’s report, Perinatal Services and Outcomes in Manitoba by Heaman et al. (2012). It highlights the sociodemographic factors associated with inadequate prenatal care in 2007 – 2008 to 2008 – 2009.
Through additional research, Heaman also explored why prenatal care matters in terms of fetal and newborn outcomes. If families – and in particular, pregnant individuals – are enlightened about how a lack of adequate prenatal care could translate into prenatal outcomes, they may be empowered to apply this knowledge to prenatal health care decisions. Insight into the longer-term implications associated with these prenatal outcomes is also important. Listen as Heaman describes what her research revealed.
Prenatal care has been shown to improve fetal outcomes. Read more about the significance of prenatal care under the subheading “Prenatal care” on pages 50 & 52 of the 2009 Report on The State of Public Health in Canada, in “Chapter 5: “Setting Trajectories for a Healthy Life”, by David Butler-Jones, then Chief Pubic Health Officer of Canada.
Barriers to accessing prenatal care can potentially be overcome if they are better understood. Besides interesting population factors associated with inadequate antenatal care, Heaman’s research found there were some personal barriers to accessing care.
Healthcare systems can also present barriers to accessing prenatal care. Watch Heaman’s next video to hear what her work revealed about the types of barriers that were identified within health care systems themselves.

Challenges experienced in accessing antenatal care vary across regions and cultural contexts. According to two sources, the Nepal Demographic and Health Survey 2011 and Simkhada et al., both cited in a review article by Joshi et al. (2013), in Nepal, of the 15% of Nepalese women who had no prenatal care, the following were identified as barriers: “…shyness towards male health workers, restriction on mobility for women, need not perceived by husband’s family or due to financial and transport constraints” (p. 248). They go on to explain it is not uncommon for women to lack knowledge about which prenatal health care services are needed or what is available to them. Furthermore, they state even when prenatal women do access care in Nepal, many will not have an awareness of prenatal factors that can affect neonatal risk, such as: pregnancy warning signs that may indicate problems, smoking or alcohol consumption or maternal diet.
Population health
Prenatal morbidity and mortality differences exist not only between various groups related to geographic location and socioeconomics, but also across determinants of health like racism. Read how social determinants affect health in Indigenous populations in the Pathways to Improving Well-being for Indigenous Peoples: How Living Conditions Decide Health report by Reading and Halseth (2013) on the National Collaborating Centre for Indigenous Health website. As you read, consider how Indigenous determinants of health like colonialism, racism and social exclusion (Reading & Wien, 2009/2013) impact the health and well-being of Indigenous peoples and what actions can be taken to improve various influences on well-being. Background information about the social gradient and how it impacts health is presented on pages 7-8. An interesting “Early Life” section follows on pages 21-26, including prenatal epidemiology about tobacco smoking, drugs and alcohol behaviours as well as the health-promoting practice of breastfeeding in this population.
Dr. Wanda Phillips-Beck, nurse research manager, First Nations Health and Social Secretariat of Manitoba, was also nurse program advisor for the Strengthening Families program in First Nations communities within Manitoba. Listen as she reveals research findings about the timing of breastfeeding decisions. The Strengthening Families program conducted this research along with Dr. Rachel Eni at the University of Manitoba.
The influence of various social determinants is often interwoven, deeply embedded in societies, and can ultimately lead to the presentation of a very unique looking piece of fabric we call “health” in populations around the world. Watch as the late Dr. Clyde Hertzman, founding director of the Human Early Learning Program (HELP) at the University of British Columbia, a former Professor in the School of Population and Public Health at the University of British Columbia, explains the concept of relational community.
Hertzman commends Cuba as a positive example in how it has demonstrated value for women, reflected in the country’s child development outcomes despite its socioeconomic challenges. Some of the positive health and education practices happening in Cuba related to prenatal care are featured in the next video excerpt from Educate your Child: Cuba’s Integrated Early Childhood Program.

What are your thoughts about government support in Cuba for women and child development from this glimpse into their prenatal health system?
According to Keon (2009), when the Canadian Senate Subcommittee on Population Health travelled to Cuba to find out more about their child development success story, one interesting finding noted polyclinic staff use their preventative and scientific approach even prior to conception. Keon states people who are at risk for less than optimal prenatal outcomes (e.g., preexisting diabetes or hypertension) are identified through standard surveillance. Primary care staff work in partnership with those identified at a higher level of risk who are interested in becoming pregnant. In this way, people are able to work towards achieving a more optimal physical status to promote better outcomes with additional support, even prior to conception.
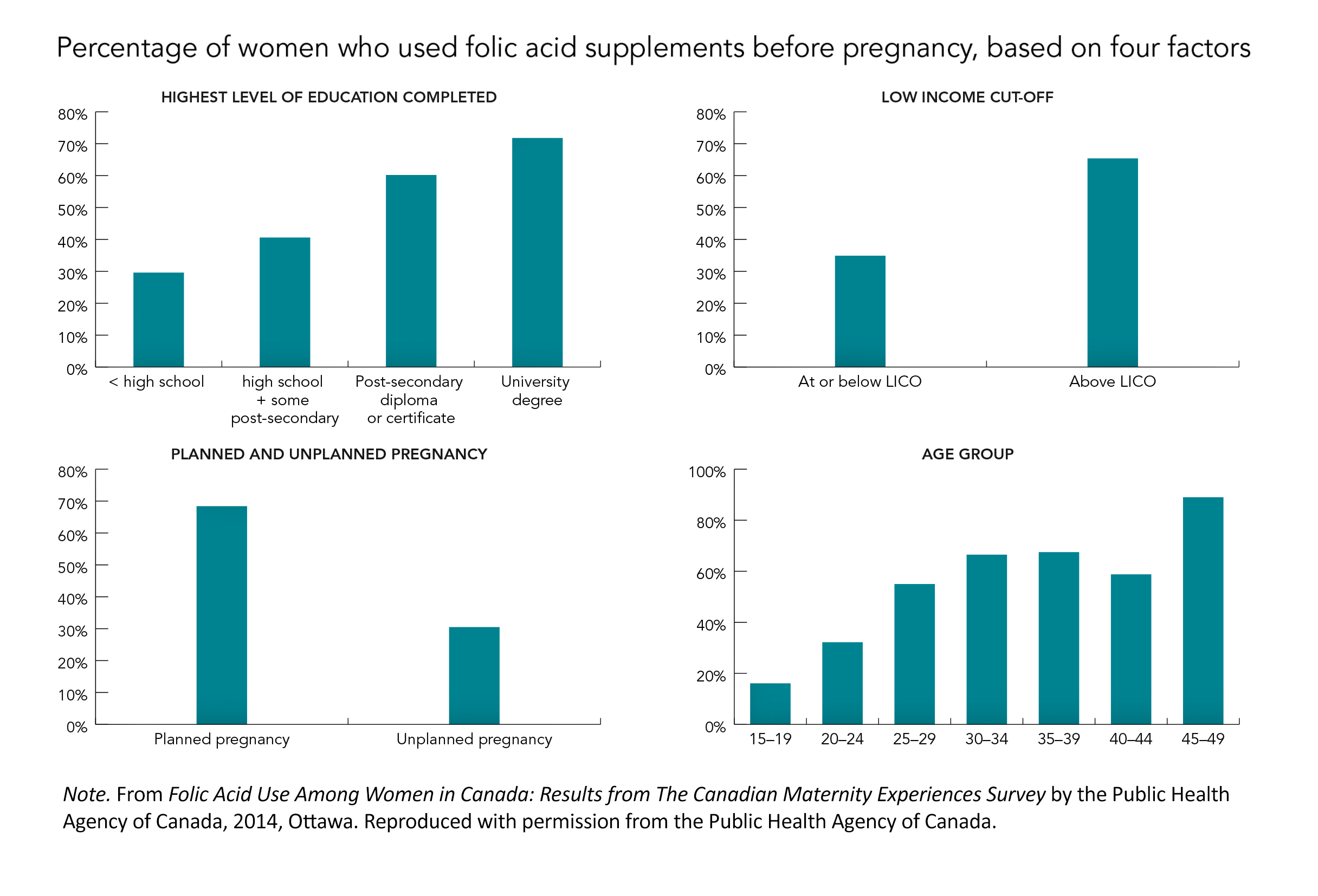
Population differences exist within Canada related to gestational parent use of folic acid supplementation before and during pregnancy, according to findings from the Canadian Maternity Experiences Survey.
Folic acid is essential for the healthy development of a fetus, particularly in preventing neural tube defects, which affect the brain and spinal cord development. These defects occur very early in pregnancy when the neural tube does not close properly and can result in serious conditions known as spina bifida or anencephaly. Because this development happens before many individuals realize they are pregnant, a daily folic acid supplement of 0.4mg should be taken through a prenatal vitamin before conception and in early pregnancy. It is recommended to begin supplementation at least three months prior to pregnancy, or as soon as possible if pregnancy is unplanned or already underway, and to continue throughout pregnancy and breastfeeding (PHAC, 2025).
The following graphs reproduced from the fact sheet Folic Acid Use Among Women in Canada: Results from the Canadian Maternity Experiences Survey (PHAC, 2014a) outline some social factor differences that were found regarding preconception use of folic acid supplementation within the Canadian population.
Additionally, a study by Yang et al. (2025) for Statistics Canada explored folic acid-containing supplement use among Canadian-born and immigrant women aged 15 to 55 years, from 2015 to 2018, and 2021. Folic acid supplement use among women of reproductive age in Canada remains relatively low, with about one in five Canadian-born women and one in four immigrant women reporting use at the time of the survey. Among those who had recently given birth, pre-pregnancy use was more common, with nearly 70% of Canadian-born women taking supplements compared to about 50% of immigrant women from regions such as West Asia, Central Asia, and the Middle East.
Awareness of folic acid’s role in preventing birth defects is a key factor influencing supplement use. However, this awareness is lower among immigrant women (65.2%) compared to Canadian-born women (80.8%). There is also considerable variation within immigrant groups, with awareness ranging from very high among women from Northern Europe to much lower among those from Southern Europe. Overall, differences in knowledge appear to play an important role in patterns of folic acid use across populations (para. 1).
What stands out for you regarding social factors and folic acid use prior to pregnancy?
Were you aware of why folic acid supplementation is important for gestational parents during the preconception and prenatal periods?
Do you have ideas for how to get this information out to more Canadians?
To discover more interesting findings from the Canadian Maternity Experiences Survey, explore the following links to the Public Health Agency of Canada website.
Preconception care
Anticipatory guidance about upcoming stages of development are windows of opportunity for influencing health decisions and future practices through education. Consider what prenatal content might be most significant for people to learn during the preconception period as Dr. Robin Williams, former associate chief medical officer of health for Ontario, discusses the concept of preconception care.
Read highlights about preconception knowledge and behaviour from a 2008 Ontario survey in the report Preconception health: Awareness and behaviours in Ontario (2009) available for download on the Best Start Resource Centre website. Focus on sections 2.1 to 2.4, found on pages 6-8 of the report.
Preconception health: What does this really mean?
Public Health Agency of Canada [PHAC] (2021) promotes a couple-based approach to preconception care, meaning both women and men are involved in preparing for pregnancy. This approach emphasizes shared responsibility for optimizing health before conception to improve outcomes for both pregnant individual and offspring. Male health is included because sperm quality and overall paternal health influence fertilization, embryo development, and pregnancy outcomes. For example, a review of research by Carter et al. (2023) demonstrated that lifestyle and environmental exposures in men can affect fetal and child health. Some modifiable risk factors included BMI, smoking, cannabis, alcohol, nutrition, physical activity and stress to improve fetal and childhood outcomes. Overall, improving the health of both partners has the potential to improve fetal and childhood development (PHAC, 2021).
Pregnancyinfo.ca is an evidence-based website that is an initiative of the Society of Obstetricians and Gynaecologists of Canada. Read the tab “Before you conceive”.

