1.1 Womb as environment
It has become increasingly clear that the placenta, far from being a passive conduit, plays a key role in the control of fetal growth” (Ross, Ervin & Novak, 2012, p. 23).
The placenta
The placenta develops within the uterus of a pregnant person. Very early in prenatal development, the zygote develops into a blastocyst which has an outer layer of cells, called trophoblasts, as well as an inner cell mass. This inner cell mass is what will develop into the embryo. The trophoblast will attach to the rich endometrium of the uterus and eventually form the placenta (King, Davidson, Avery & Anderson, 2015, p. 605).
During the second month of a pregnancy, a complex system of blood vessels is already functioning within the placenta that allows for exchange of gas, nutrients and waste between the embryo and its mother (Moore & Persaud, 2008, p. 72). In the video below, Dr. Alan Bocking, Professor in the Department of Obstetrics and Gynaecology at the University of Toronto, explains more about the main functions of the placenta.
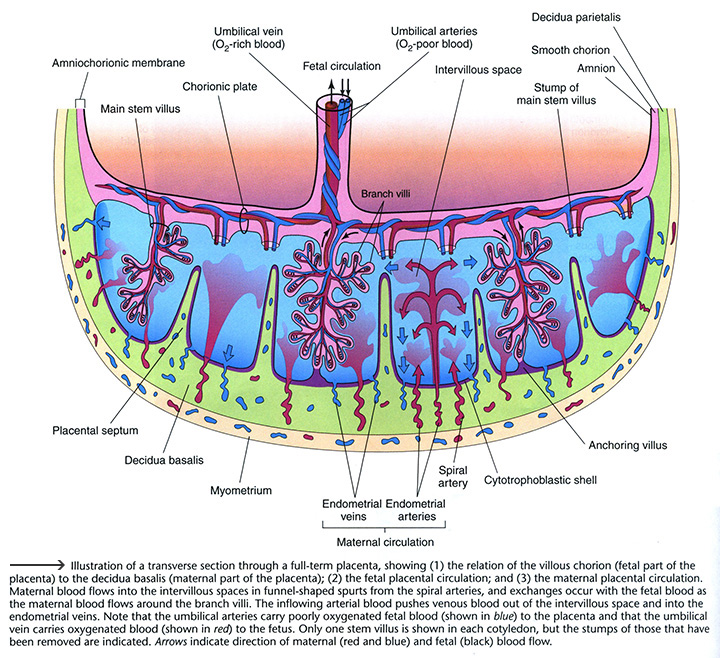
Visualize from the diagram below how blood flows through a fully developed placenta. Some of the main processes which occur through this system involve transfer of oxygen and nutrients from the mother to the fetus and waste and carbon dioxide from the fetus to the mother.
Find out more about these remarkable functions of the placenta on the Mount Sinai Hospital website.
Alan Bocking describes the placenta as an “incredibly impressive endocrine organ”. Play the “Build a Baby” game to learn about the four main hormones produced by the placenta and how they work to support pregnancy.
As an essential organ which only develops during pregnancy, the placenta plays a crucial role in the quality of the intrauterine environment experienced by the developing fetus. The placenta is capable of adapting its function to a variety of conditions as it integrates chemical messages from the mother and the fetus. (King et al., 2015, p. 606).
How well the placenta is able to develop and function has important implications for fetal growth and development. Listen as Dr. Stephen Lye explains more about these implications.
Moffett-King, A. (2002), Natural killer cells and pregnancy, Nature Reviews Immunology, 2, 656-663. doi: 10.1038/nri886 Retrieved from http://www.cvs.ed.ac.uk/sites/default/files/A%20Moffett-King_0.pdf
Copyright 2002.
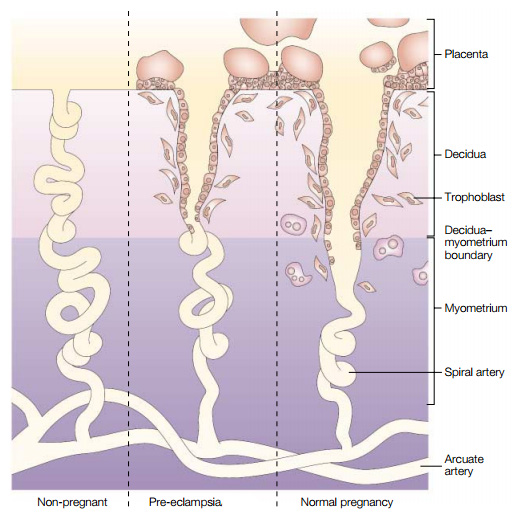
According to Moore and Persaud (2008), 80 – 100 spiral arteries are found within the decidua basalis (a maternal part of the placenta seen in the first diagram on the page). Maternal blood flows from these spiral arteries into the intervillous space. Exchange of products with the fetus occurs as maternal blood flows more slowly around the branch villi (p. 75). In the second diagram on the page, note the variance in quality of maternal spiral artery invasion from trophoblast cells that may occur during pregnancy. With preeclampsia, the condition mentioned in the preceding video, this invasion occurs at a superficial level. In a normal pregnancy, the trophoblast cells invade into the myometrial, not just the decidual portion of these blood vessels and transform the spiral arteries into more open vessels. The structural changes in this healthier invasion accommodate a significant increase in uterine blood flow (optimizing the volume of blood flowing through this location in the fetal supply line) (King et al., 2015, p. 606).
Maternal conditions such as diabetes or hypertension may decrease the flow of blood from the uterus to the placenta – if the mother’s uterine spiral arteries have been affected by these disease processes (King et al., 2015, p. 614). Other examples of factors outlined by Blackburn (2013) that may alter uteroplacental blood flow include maternal behaviours (smoking or drugs) and even physical or emotional stress (p. 96). Importantly, when there is a decreased functional ability by the placenta to provide for fetal needs – due to reduction of blood flow or other factors – fetal growth restriction can occur. Listen to the next video as Dr. Maggie Morris describes how smoking impacts placental function.
View | Morris – smoking and the placenta (1:23) Not available in this preview
Read more about how smoking in pregnancy can affect the mother and fetus in the following synthesis of information on the Encyclopedia on Early Childhood Development website.
Stress in the womb
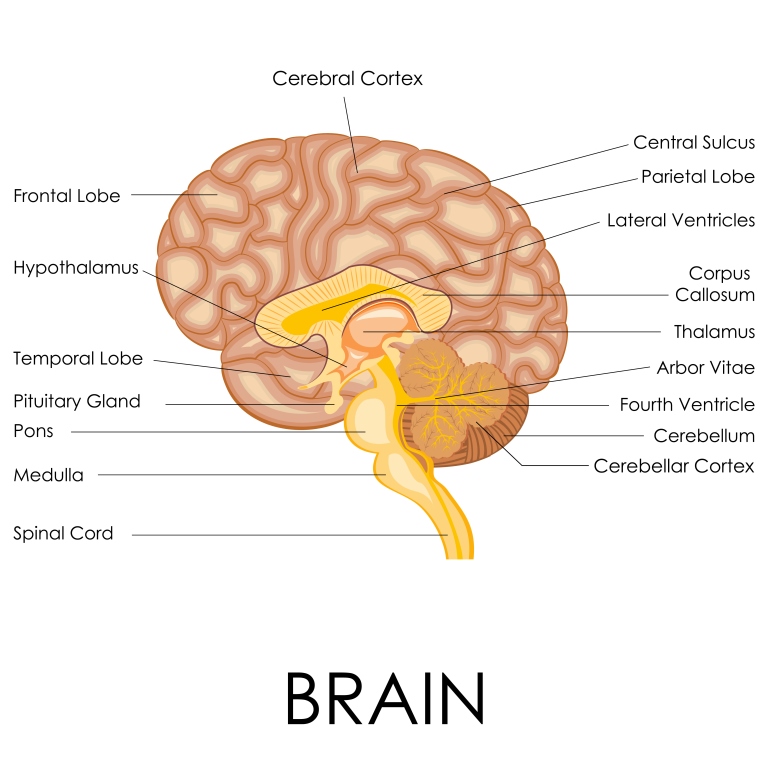
The body has an incredible response system to help it cope with stressors. One part of this system is the hypothalamic-pituitary-adrenal (HPA) axis. The hypothalamus, located in the forebrain, is situated just above the pituitary gland and helps the body maintain internal balance. It functions as a link between the nervous and endocrine systems. Watch the “Endocrine system” video from the MedlinePlus webpage on “Endocrine glands” to see how the nervous and endocrine systems work together to maintain equilibrium within the body.
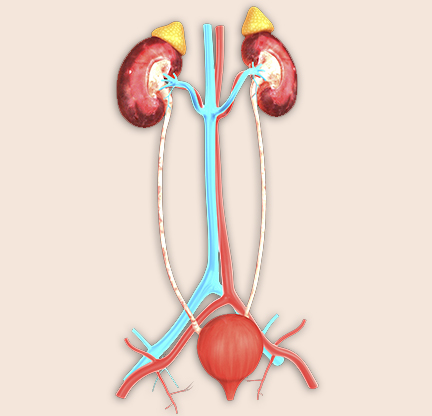
In the image at right, note the adrenal glands, a set of triangular shaped glands that belong to the endocrine system, situated at the top of each kidney. Cortisol, a glucocorticoid hormone, is produced by the adrenal cortex (the outer segment of these glands) in response to either physical or psychological stress. Dr. Joanne Weinberg, Professor and Distinguished University Scholar in the Department of Cellular & Physiological Sciences at the University of British Columbia, explains how the HPA axis works both in response to stress and in situations of normal daily living.
Glucocorticoids are essential for life, influencing virtually every tissue and affecting a wide range of physiological functions from metabolism, blood pressure, the immune system, regulation of fluid and electrolyte homeostasis and increasing energy demands in response to stress” (Reynolds, 2013, p. 3).
Click through the next interactive activity to learn more about how the HPA axis works as a negative feedback system to help the body cope with more acute stressors.
Interact | HPA Axis Not available in this preview
According to McEwen and Gianaros (2011), the HPA axis is one of the biological systems that may provide protection and benefit to various body systems when activated as required and subsequently terminated quickly and appropriately (p.433). For example, memory may be improved in part from the release of cortisol in a threatening situation, which may better enable an individual to avoid danger in the future (McEwen, 2005, p.317). However, as discussed by Joanne Weinberg in the previous video, if a stressor were to become repeated or chronic, the prolonged activation of the HPA axis could result in more negative effects, such as illness related to suppression of the immune system. In the example of memory, which may be improved in a short term stressful situation, impairment might develop if the stress were to occur repeatedly over time (Roozendaal; McEwen as cited in McEwen, 2005, p.317). Increasing wear and tear over time on the brain and body systems from chronic stress may undermine an individual’s physical and mental health (McEwen as cited in McEwen, 2013, p.674).
In the next video, Dr. Brandy Wicklow describes fetal development of the HPA axis, which will become the lifelong regulator of cortisol secretion.
View | Wicklow – fetal HPA axis development (2:16) Not available in this preview
Ross and Desai (2012) explain that for normal prenatal maturation and development of organs such as the kidneys, lungs and brain to occur, the fetus needs steroid hormones (e.g., the glucocorticoid hormone cortisol). They also point out that starting from midgestation, glucocorticoid receptors are expressed in most fetal tissues. The diagram of the brain presented earlier within the interactive activity shows the location of the hippocampus, an area known to have numerous glucocorticoid receptors. Learning and memory are important functions associated with the hippocampus (Ross & Desai, 2012, p. 91).
In the next video, Dr. Stephen Matthews explains more about maternal prenatal adversity, revealing that glucocorticoids are linked with programming of how the fetus functions after birth.
View | Matthews – maternal adversity (2:25) Not available in this preview
In the review article “Glucocorticoids and Fetal Programming Part 1: Outcomes”, Moisiadis and Matthews (2014a) describe how mounting scientific evidence supports the hypothesis that raised fetal cortisol levels associated with stress induced increases in maternal cortisol, can affect fetal neurological (brain) development as well as the function of the HPA axis after birth (pp. 397-398). They state conditions of maternal adversity such as depression, anxiety or undernutrition may result in increased levels of glucocorticoids within the mother and fetus (p.391). Additionally, they indicate physical stressors such as fetal hypoxia (lack of sufficient oxygen supply to its tissues) may also result in increased fetal glucocorticoid levels (p.391). A final originating cause of elevated fetal glucocorticoid levels internal to the maternal-fetal-placental unit could occur when higher glucocorticoid levels in the maternal circulatory system are present and the placenta is not functioning adequately in its protective role (Chapman, Holmes & Seckl as cited in Moisiadis & Matthews, 2014a, pp. 391-392).
Importantly, alterations in the set-point of the HPA axis during prenatal development from exposure to excessive glucocorticoids may result in changes to offspring HPA axis activity even into adulthood (Reynolds, 2013, p. 5). McGowan and Matthews (2018) point out the relationship between maternal prenatal adversity, fetal exposure to glucocorticoids, and subsequent effects on HPA axis function and reactivity to stress post-birth is complex. In their mini-review, they report factors such as the type and timing of prenatal adversity, offspring sex, context of the post-birth stressor activating the HPA axis as well as the age of the infant or child may all be contributing factors in how the HPA axis functions and how the infant or child responds to stress. Positive environmental influences may also impact earlier stress effects. For instance,Lupien, McEwen, Gunnar and Heim (2009) report there is now evidence that the quality of care received by a newborn after birth often influences the strength of the effects of prenatal stress. This evidence underscores the continuing plasticity of the brain during development in the postnatal period (p. 436).

The coping techniques and strategies people use to manage challenges or stressors can vary greatly. If viewed on a scale, one end may show positive health-enhancing behaviours, while the other end shows behaviours associated with health risk-taking. According to the Public Health Agency of Canada (n.d.-c), social relationships and belonging, stress, sense of control, culture and personal life skills are key areas through which combined social and economic environmental forces exert a strong influence on an individual’s lifestyle choices. Listen as Monica, a married working mother of two children, reveals how she takes care of herself now that she is in the 28th week of her third pregnancy.
What self care strategies is Monica using to help maintain a sense of balance in her life?
How might self-care strategies influence fetal development?
What are some examples of environmental influences that support a sense of balance in daily living?
Can you identify some personal health practices that you engage in for your own social, emotional or physical well-being?
For more information on how the development of the brain and function after birth can be programmed during the prenatal period, read Working Papers #3 and #10 by the National Scientific Council on the Developing Child on Harvard University’s website for the Center on the Developing Child.
Developmental origins of health and disease
Some earlier epidemiological work by Dr. David Barker began the “fetal origins” of adult disease hypothesis. His work noted associations between low birth weight of offspring and later adult onset of coronary heart disease. This hypothesis has more recently come to be understood as the developmental origins of health and disease. In the following video, Sir Peter Gluckman defines our current understanding of this concept.
Since the initial focus on adult onset of cardiovascular disease, evidence has grown to expand the list of health conditions that may trace back to developmental origins. For instance, Barouki, Gluckman, Grandjean, Hanson and Hinder (2012) indicate a variety of health conditions may be linked in part to developmental nutritional or chemical exposures. Examples of these conditions include: asthma and allergies, diabetes, obesity, hypertension, osteoporosis, schizophrenia, depression, neurodevelopmental disorders (e.g., learning disorders), neurodegenerative diseases, and some cancers (Background section, para. 6). In association with fetal and early life “programming” experiences, some health conditions have also been noted to surface as early as childhood (Moisiadis & Matthews, 2014a, p. 391).

Scientists have discovered it is not only low birth weight, but also high birth weight that increases risk for future disease. In fact, “epidemiologic studies have confirmed that the relationship between birth weight and adult obesity, cardiovascular disease, and/or insulin resistance is in fact a U-shaped curve, with increasing risks at both the low and high ends of birth weight” (Ross & Desai, 2012, p. 86). Importantly, the risk for disease is on a continuum so that even when birth weight remains within a normal range as an outcome of pregnancy, experiences – for example, chemical exposures or nutritional imbalance during fetal life – may still have programmed an increased risk for later onset of disease within offspring (Barouki et al., 2012, “Developmental nutrient and toxicant exposures” para. 5). Besides the nutritional environment that is provided for the developing organism, maternal metabolic and hormonal environments can also contribute to the quality of embryo or fetal experiences within the womb. Possible effects on offspring metabolism and physiology from these types of gene by environment interactions during prenatal development can occur through permanent modifications to cellular responses, organ structures and gene expression (Ross & Desai, 2012, p. 84).
In the following diagram, click each organ or tissue type to see examples of how they may be potentially programmed during prenatal development towards an increased risk for disease. You will note that both the liver and pancreas have additional audio icons, where you can hear Dr. Daniel Hardy, Associate Professor from Western University, explain in more depth why these organs, (which may be seen as less important in their functions relative to the brain or the heart), are still important organs to study in regards to fetal programming.
One of the ways programming of function towards an increased risk for disease may occur prenatally is through epigenetics. Watch as Dr. Michael Skinner, Professor in the School of Biological Sciences at Washington State University describes what epigenetics is and how risk for disease can be programmed in early prenatal development.
View | Skinner – epigenetics from conception (4:07) Not available in this preview
Dr. Skinner mentions the epigenetic mechanism known as DNA methylation in the previous video. Listen as Dr. Meaghan Jones explains more about DNA methylation.
View | Jones – DNA methylation (1:22) Not available in this preview
Next Dr. Jones describes a prism model she developed for explaining the role of epigenetics in the Developmental Origins of Health and Disease [DOHaD] hypothesis. Ultimately, it helps us to visualize how there can be a shift in the potential range of one’s risk or opportunity for later health outcomes due to early developmental exposures.
View | Jones – prism model (3:32) Not available in this preview
Watch as Sir Peter Gluckman describes what we are learning about epigenetics in the prenatal period of development. He reveals some of the more recent discoveries about prenatal factors and experiences that may increase risk for future disease.
Part of our expanded understanding from the fetal origins hypothesis relates to what is being discovered about the evolutionary aspects of fetal programming. In the next video, Meaghan Jones explains intergenerational transmission as a way to help the fetus prepare for its future interactions in the world.
View | Jones – intergenerational transmission (1:15) Not available in this preview
Listen as Stephen Matthews describes the concepts of “Predictive Adaptive Response” and “Mismatch” which take into consideration the postnatal environment into which an infant is born.
View | Matthews – Predictive Adaptive Response & Mismatch (2:51) Not available in this preview
Another example is provided by Stephen Lye of how physiologic adaptations made during prenatal development can become maladaptive and increase risk for disease when there is a significant mismatch between the prenatal and postnatal environments.
View | Lye – physiologic mismatch (2:39) Not available in this preview
Recall the pre-pregnancy period was also mentioned as a time of influence on the next generation’s health and well-being in Sir Gluckman’s first video in this section. To learn more about how this time period relates to future offspring well-being, read the first article “Before the Beginning: Nutrition and Lifestyle in the Preconception Period and its Importance for Future Health“ by Stephenson et al. (2018) in a series on “Preconception Health” on The Lancet website. You may register for free access to the full text on The Lancet website (or you might have access through your library).

